Best Practices for EBT

This article aims to help the reader avoid the simple mistakes that many organisations are making in the rush to implement thermal imaging technology for fever screening. It is far from comprehensive but aims to provide a high-level overview of how thermal imaging technology can be used effectively.
How the camera can detect fever:
- The camera can be used to measure the temperature of the region medially adjacent to the inner canthus of the eye (inner corner of the eye)
- This region is directly over the internal carotid artery
- The current evidence states that this area is preferred for fever screening due to the stability of measurement
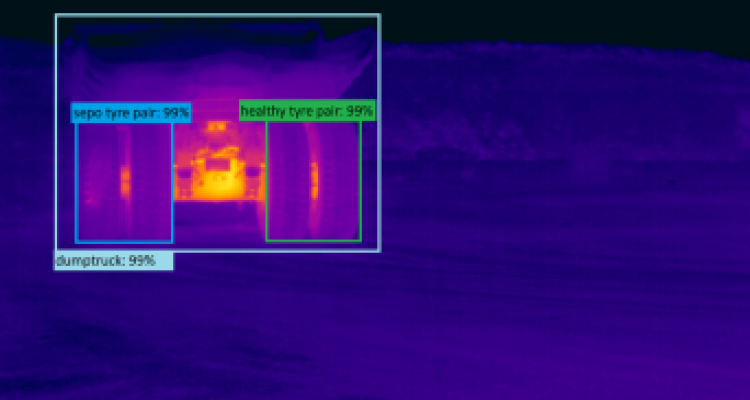
Firstly, this means that 90% of the content showing up on the internet should be disregarded. It is simply not possible to measure the temperature of the canthi of 15 people from across a room with any technology available today.
The “AI-based COVID-19 detection cameras" that are being marketed heavily are mostly just a cash grab by organisations capitalising on fear. They are dangerous, as they are leading organisations to believe that they have effective systems and protection for their workforce in place. In fact, this equipment will be ineffective and do little other than provide a false sense of security.
For a more detailed explanation, please see the article here.
Consistency and repeatability is the key to getting good results for this application. Handheld style thermal cameras must be tripod mounted. If used in a handheld fashion they are likely to give inconsistent results, especially when operated by staff without appropriate training. However, even trained thermographers would find it challenging using a handheld camera for this application. Low-cost handheld thermal cameras exacerbate this problem.
Key Considerations
Effectively implementing thermography for fever screening is not a trivial process. Consideration needs to be given to many aspects of the screening process. Some of the key considerations and general notes are captured below.
Operating environment
- The screening station should be located near the entrance to the site, to minimise the potential interactions of any infected individual
- Indoors or a well-covered/protected area to meet the below requirements
- Minimal airflow, i.e. not under an air conditioner duct or with a crosswind
- Climate controlled, ideally 20 °C to 24 °C and relative humidity <50 %
- Non-reflective background, a light colour matte finish wall is fine
- No thermal radiation sources, i.e. no reflections from the sun, hot/cold external windows, hot halogen lamps overhead etc
- Do not place the screening system near bathrooms, a wet face will alter the measurements
Secondary screening
- The camera is not diagnosing any medical condition, it is only identifying a potential elevated body temperature (EBT)
- If someone is identified to have an EBT, qualified medical personnel need to assess the individual using a clinical thermometer, in a secondary screening area
- This should be positioned to allow the removal of an individual with an EBT from the facility with reasonable privacy and with minimum potential for cross-contamination of others

Workflow
- Individuals must stop/pause in front of the camera one at a time. The screening process should take <1 second once the face is stationary in front of the camera
- The camera is aligned straight on to the face (both horizontal and vertical), you may need to allow for height adjustment of the camera for tall/short individuals.
- The individual needs to look straight at the camera, not look up, down or to the side
- Remove hats, glasses, goggles, hair covering eyes etc a clear line of sight to the face/eyes is required
- Consistent distance between the camera and the face of all individuals. Mark a line or feet marks on the ground.
- The distance needs to be set based on camera resolution and lens angle. See the section below on camera hardware.
- Emissivity set to 0.98, distance to the target and environmental parameters set correctly.
- Both the target region for the face and the target region for the blackbody reference should have correct parameters set individually
- The responsible organization should consult their medical advisor on the setting of the threshold temperature. An example threshold temperature may be >37.4°C.
Notes on equipment selection
Camera hardware
- Uncooled microbolometer long-wave infrared thermal imaging camera with a minimum 320x240 pixel resolution
- Focusable lens, not a “focus-free” camera
- Pixel size (iFoV) at the distance of measurement ≤1mm
- For a 320x240 camera, this means the face must cover >75% of the width of the image
- The NETD of the camera should be ≤50mK (MRTD <100mK)
- Measurement uncertainty less than ±0.5°C between 34°C and 39°C. This is the total "system" offset error and includes uncertainty in the reference source. (see IEC 80601-2-59, 201.101.2.2)
- Please see this article for common lens calculation tables
- Allow the camera to stabilise at operating temperature prior to starting screening, i.e. leave turned on for >30 minutes prior to starting
- Stable mounting of the camera, such as a sturdy tripod
Blackbody reference source
- The centre uniform region of the blackbody needs to be large enough for a 20x20 pixel area box to be set up (i.e. larger than 20mm x 20mm, a 50mm diameter blackbody is ideal)
- Needs to be placed at the same distance from the camera as the individual's face
- Technical specifications:
- Known radiance temperature within the range of 33 °C to 40 °C
- Uncertainty of less than ± 0.3°C
- Combined stability and drift of less than ± 0.1°C, over an interval of more than 14 days
- Emissivity of ≥0.98
- Temperature uniformity better than 0.2 °C
The scanning station requires the camera to be horizontal, with both the face and blackbody reference in sharp focus. The backdrop should be a flat, non-reflective surface.

Summary
In summary, there are lots of people being tasked by their organisation to “buy a thermal camera to do fever screening, like the one I saw on YouTube”. If you are the person who has been tasked with this, please take the time to research the requirements for the system. Having no system at all is better than a system that does not work correctly. At a minimum the organisation has the following responsibilities:
- Purchase appropriate equipment that is fit for purpose
- Ensure periodic QA, maintenance and calibration of equipment
- Define how/when/where of the screening process
- Critically, no camera can provide a medical diagnosis. It is simply indicating that an individual may have an elevated body temperature. The organisation needs to carefully consider how any EBT detection will be managed.
- Provide appropriate operator training
- Appropriately manage the storage of any screening data that is captured
- Many more as defined within the relevant standards and acts
We hope that these articles can help people to make more informed decisions when implementing thermal imaging technology for fever screening. The next article will cover some common lens angle calculations that need to be made.